Understanding postpartum psychosis: A survey and expert perspective
Delve into the realities of postpartum mental health through our comprehensive survey findings and an insightful interview with a leading psychiatric nurse practitioner. Gain a deeper understanding of postpartum psychosis and its impact.

Survey insights on postpartum experiences
We conducted a comprehensive survey with 25 questions to gather critical data on postpartum mental health. The survey explored various aspects including consent, age, origin, race, gender, number of pregnancies, recent childbirth within the last 12 months, and the presence and type of mental health symptoms experienced post-delivery. It also investigated whether participants received a diagnosis of Postpartum Psychosis and if their pregnancy was planned.
Participants ranged in age from 22 to over 50. The demographic breakdown included 10% identifying as Hispanic, Latino, or of Spanish origin, 80% as White females, and 10% as Black or African American. Regarding family size, 30% had one child, 40% had two, 10% had three, 10% had four, and 10% had five children.
- 80% of the participants experienced complications during birth
- 60% of the participants gave birth vaginally, 40% gave birth via C-section
- All participants rated their sleep quality after birth poorly
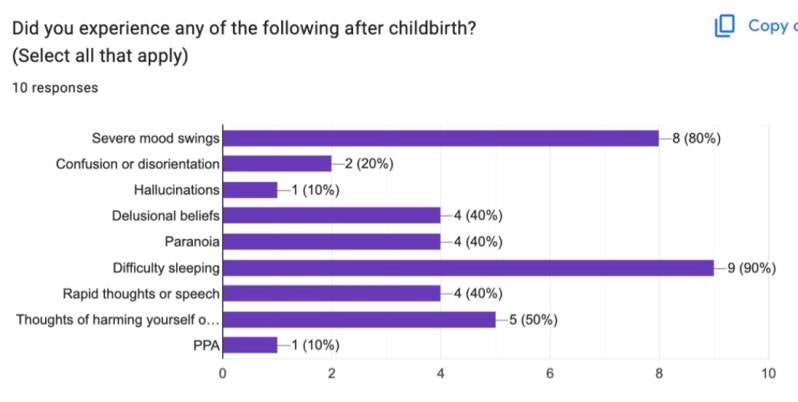
- 80% of participants experienced mood swings, 20% experienced confusion or distortion,
10% experienced hallucinations, 40% experienced delusional beliefs, paranoia, rapid
thoughts, 50% experienced thoughts of harming themselves, and 10% experienced Post
Partum Anxiety.
- The range of symptoms began immediately to 6 months after giving birth.
- The duration of symptoms ranged from 3 months to 2 years
- 100% of participants sought medical help
- The duration it took to receive a medical diagnosis ranged from 6 weeks after birth to 2
years
- 80% of participants took medication for treatment, and 90% recieved therapy
- When asked to rate if treatment helped on a scale of 1-5 (1 being no, 5 being yes), 10%
rated it a 2, 10% rated a 3, 20% rated a 4, and 60% rated a 5.
- 70% of participants felt supported by loved ones
- When asked about barriers, 100% said mental health, 60% said daily functioning, and
40% said building a relationship with their baby
- When asked if they felt if they were properly informed about the risks of PPP, 60% said
no
- One participant mentioned that they were not screened for depression in any follow-up
appointment

An expert perspective: Interview with Amber Conway
Following our survey, we conducted an insightful interview with Amber Conway, a Psychiatric Nurse Practitioner (MSN, BSN). This discussion focused on her professional views and experiences concerning postpartum psychosis, offering invaluable insights into the diagnosis, treatment, and support for individuals affected by this condition.
Her expertise sheds light on the critical aspects of care and awareness surrounding postpartum mental health, complementing the quantitative data gathered from our survey. Her perspective emphasizes the importance of early detection and intervention.
1. How would you explain postpartum psychosis to someone with no medical background?
- Post partum psychosis is a mental health crisis that emerges after birth. It is rare
but severe. It significantly impairs judgment, perception, behavior, and decision-
making. It requires urgent medical intervention and common symptoms include:
extreme confusion or disorientation, severe mood swings, paranoia or intense
suspicion, hearing voices or seeing things that aren’t there, false beliefs/delusions,
rapid speech or racing thoughts, agitation or unusual behavior, not sleeping for
long periods (this is one of the first symptoms we look for because lack of sleep
can cause anyone to go into psychosis, and/of thoughts of harming self or baby.
2. How is it different from postpartum depression?
- The short answer: Postpartum depression affects mood; postpartum psychosis
affects reality. The longer explanation is that each have a different period of
onset. Post partum depression is usually weeks to months after birth and is more
common while PPP is sudden to weeks after birth and rarer. With postpartum depression, the mom may experience deep sadness, numbness, constant worry,
shame, guilt, exhaustion, feelings of being a bad parent, and difficulty enjoying anything. She usually knows that these feelings are happening and are often very distressed by them.
- With postpartum psychosis, mom may believe things that are not true, hear or see
things others do not, become intensely suspicious, go without sleep while feeling
highly energized or frantic, talk rapidly or incoherently, seem like a completely
different person or become confused and disconnected from reality. She may not
(usually does not) realize that she is mentally unwell.
3. What are the earliest warning signs families should watch for?
- First sign is lack of sleep (significant lack) but not being overly tired or exhausted
from the lack of sleep. Person would display heightened energy, pressured speech, rapid/racing thoughts (but you may not “see” this), isolating, being extremely
paranoid or suspicious (think not allowing anyone other than themselves to care for baby because they can’t do it correctly or something will happen if mom isn’t
the one to watch and care for the baby 100 percent of the time) and extreme moodiness and agitation.
4. What types of patients are most at risk for developing postpartum psychosis?
- Those with a history or family history of Bipolar, history of PPP, extreme sleep deprivation after birth (think colicky baby who doesn’t sleep and cries non-stop-
mom never gets a break), patients who were on mood stabilizers prior to pregnancy but had to come off due to pregnancy (we typically attempt to get them
back on their meds ASAP after birth to negate the chances of PPP and we watch them more closely as well—BUT that would be for patients in our care. First time moms may not have this advantage and be more susceptible to PPP).
5. How do you assess and diagnose a new mother who may be experiencing it?
- To diagnose we use numerous avenues- blood tests to rule out any type of
infection or thyroid issue (which can mimic some of the symptoms), neurologic assessment, then psych screening to include mood, perception, assess for
hallucinations both auditory and visual, sleep pattern (amount per night, difficulty falling or staying asleep), past psych history, and onset (remember timeline of
onset does matter). Collaboration with OB is essential as they may be the first touch with these patients at their follow up appointment.
6. What does a typical treatment plan look like?
- Since this is more of a mental health crisis, the mom will more than likely be
hospitalized on an inpatient behavioral health unit where experts can care for her.
One of the most critical aspects will be sleep so we usually prescribe a medication
such as Seroquel to assist as a sleep aid. This is given in conduction with an antipsychotic med and a mood stabilizer. Medications can be a wide variety and
will be prescriber dependent but our goal is safety, sleep, and stabilizing the
mood.
7. How do you handle situations where there may be safety concerns for the mother or
baby?
- Immediate safety is the key factor. Ensure spouse or grandparents are aware and
can help with baby, ER visit/INPT admission as indicated, CPS if warranted,
remove objects from home that may cause safety concern (knives, firearms), do not leave mom alone with baby/other children until mood is stabilized and crisis
is over.
8. How should family members respond if they suspect postpartum psychosis?
- Take the symptoms seriously, do not leave mom alone with baby/other children, seek professional intervention ASAP (OB, psych provider if established prior to
pregnancy), go to ER if warranted, call the crisis hotline and try to create a low stimulus environment (as much quiet as possible, no blame, no intense conversations, relaxation techniques).
9. What barriers prevent women from getting help?
- First and foremost: stigma or fear that they will lose their baby/children. Other
obstacles for seeking treatment: early signs like lack of restorative sleep may be
seen as “normal” and delay seeking treatment, shame, guilt, family seeing this as
“normal” exhaustion or post-partum hormone fluctuations, or a “normal”
adjustment to being a new mom or exhausted mom.
10. What is the most important thing you want people to understand about postpartum
psychosis?
- Mom cannot simply “control” this situation. This is beyond her control and she
should not be judged and guilt should not be placed on her due to something that
is not within her control. It can be treated and she is a good mom. There should be
no stigma: addressing her mental health is of the utmost importance.
Create Your Own Website With Webador